Dr.Sunil Shroff, Dr.Sanjay Pandey, Dr.Georgi Abraham, Dr.P.Soundarrajan
Head of Department - Urology & Renal Transplantation,
Sri Ramachandra Medical College & Research Institution, Chennai
[email protected] or
[email protected] or
[email protected]
Introduction
The conventional surgery for removal of Continuous Peritoneal Dialysis catheter is similar to open insertion technique and requires the surgeon to either go through the same incision or make a parallel incision close to the previous scar. We describe our experience with a simpler technique of removal that involves a small incision and sustained pull and with some jerks for the removal of the catheter.
CAPD catheter removal surgery is most commonly required when there is non-resolving peritonitis (1) or catheter malfunctions or if the patient undergoes a satisfactory transplant. The complete list of indication that demand catheter removal are as follows:
Catheter Removal In Case Of Complications:
- Recurrent peritonitis.
- Persistent exit site infection
- Refractory peritonitis
- Tuberculous or fungal infection causing peritonitis
- Tunnel abscess
- Recurrent leakage of the dialysis fluid through the exit site
- Rarely in the event of persistent abdominal pain or discomfort due to catheter resting on internal organs and due to inflow of solution
Catheter Removal In Case Of Catheter Malfunction:
- In early post-operative period - Obstruction of catheter due to intra-luminal blood or fibrin clot or omental plug. Sometimes a kink along the course of catheter may cause its malfunction
- Catheter migration out of pelvis leading to poor drainage patients usually present with this problem a few months after the catheter has been inserted.
- Blockage of catheter due to adhesions that may occur after a severe episode of peritonitis.
- Very rarely a hole in the silicon rubber or breakage may require the catheter to be removed or changed.
Removal of Functioning Catheter:
- Successful renal transplantation
- Patients wanting to switch to haemodialysis.
Method
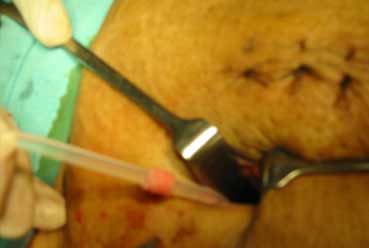
The Slow Pull and Jerk Technique: This can be performed under local anaesthesia and does not involve any open surgery. It can either be done at the patients bedside or in an operating room The comfort in the operating room is the operating light and ready availability of instruments and staff.
A small nick is made at the exit site to increase the size of the tunnel. A sustained traction is applied on the catheter till the external cuff comes out. After this the catheter is re-gripped and pulled as one gives a sustained traction the inner cuff may give way and the catheter thereafter slips out.
In some cases where the catheter has been kept for long duration the inner Dacron cuff can become part of the tissues and it does not come out but yields in such a way that the silicon catheter comes out leaving behind the Dacron cuff. If there is a problem then some blunt and sharp dissection maybe necessary to deliver the fibrous firm tissue around the inner cuff, Sometimes sharp dissection is required to divide this tissue. We have often used a no.12 blade and kept the dissection very close to the fibrous tissue. This dissection may mean some enlargement of the incision from the exit site towards the inner cuff. On the two occasions when the catheter when the has snapped in our series; it has done so just distal to the inner Dacron cuff. The wound was left to heal by secondary intention if there was an infective element, otherwise it was closed primarily.
From 1997 to 2006 we removed 43 catheters (Table.1). The indication for removal of the catheter in majority was non-resolving or recurrent peritonitis (31). In the rest it was due to post transplantation (7) or catheter mal-position & malfunction (5) (Table .2 ).
Results
39 of the 41 patients had removal of the catheter successfully using this technique; in 2 patients the catheter snapped at the peritoneal end of the Dacron cuff and these patients were converted to open removal . There we no post-operative complications. The wound healed in all the patients.
Discussion
Patients who are on long term renal replacement therapy using the CAPD as the form of dialysis may require change of catheter either due to malfunction or peritonitis(1). In this situation the repeated attempts to open the peritoneal cavity can lead to adhesions making subsequent CAPD catheter insertion difficult. A closed method for removal of the catheter prevents or lessens the problem of adhesions. Fungal peritonitis in particular entails early catheter removal with anti fungal cover and therapy to reduce mortality rates in this group (2)
The advantage of the procedure is that it takes only 10 to 15 minutes and avoids open surgery. One should remember to drain the dialysate fluid before undertaking catheter removal. Once the inner cuff come out the catheter slips out quite easily.In open surgery rarely we see the inner section of the catheter adherent to bowel or peritoneum and there maybe some risk in pulling on such a catheter.. We have as yet never had a situation where the peritoneal section of the catheter is difficult to deliver due to adhesions. One should be careful when undertaking sharp dissection of the inner cuff area as there maybe bowel stuck to the scar. It is useful to cut on the fascia just outside the Dacron cuff and once the cuff is seen sharp dissection can be done from the lumen outwards. This lessens the risk of damage to the viscera
In our series there was only one case where the catheter had to be removed within the first three month after insertion. In two cases where the catheter snapped from the inner cuff an open technique was undertaken on the same day to remove the catheter. Post catheter removal there was no complications that were encountered except for an occasional patient who discharged some fluid from the drained site. The small peritoneal opening was closed using a few chromic catgut sutures. To help with closure the first suture was taken while the cuff was still attached partly to the peritoneum.
Most centres that we know do open surgery for its insertion or removal either under local, regional or general anaesthesia. There is paucity of peer reviewed literature on CAPD catheter removal. The surgery of CAPD catheter removal is never mentioned in standard textbooks or even in surgical manuals. However this less described procedure forms an important part of any CAPD programme..
| Year | No of CAPD Catheter Removed |
| 1997 | 1 |
| 1998 | 3 |
| 1999 | 1 |
| 2000 | 3 |
| 2001 | 3 |
| 2002 | 5 |
| 2003 | 5 |
| 2004 | 6 |
| 2005 | 14 |
| 2006 | 2 |
| Total | 43 |
Table.1. Year-wise data on removal of CAPD Catheter
| Non-resolving Peritonitis | 31 |
| Transplantation | 07 |
| Catheter Migration & malfunction | 05 |
| Total | 43 |
Table 2. Indications for Removal of Catheter
Reference
- Garcia-Martinez MC,Leonos Mirinda A, Factors associated with peritoneal dialysis catheter failure in chronic renal insufficiency, Rev Invest Clin 1997 May-Jun;49(3):189-95
- Nagappan R, Collins JF,Lee WT, Fungal peritonitis in continuous ambulatory peritoneal dialysis--the Auckland experience.Am J Kidney Dis ,1992 Nov;20(5):492-6

CAPD Catheter in place

Small Vertical Incision

Outer Cuff delivered by Pull & Tug Technique
Pull and Retraction for dissection of inner cuff

Both Cuff Delivered and catheter being with drawn from the peritoneal cavity

Small Scar of CAPD Catheter Removal