Dr.Sunil Shroff, Dr. S.Venkat Ramanan
Department of Urology & Renal Transplantation
Sri Ramachandra Medical College & Research Institute Porur, Chennai 600116
www.srmcurology.com, [email protected],
Tel: 044-24761546, Fax: 044-24761540.
UROFLOWMETRY
- Electronic recording of the urinary flow rate throughout the course of micturition.
- Simple, diagnostic screening procedure used to calculate the flow rate of urine over time.
- Common, non-invasive urodynamic test used in the diagnostic evaluation of patients presenting with symptoms of Bladder Outflow Obstruction (BOO).
- Results from the test can suggest if the flow is normal or abnormal. Abnormal results are nonspecific for the cause of the disease.
- Abnormally low flow rate may be caused by obstruction or detrusor hypocontractility.
Terminology
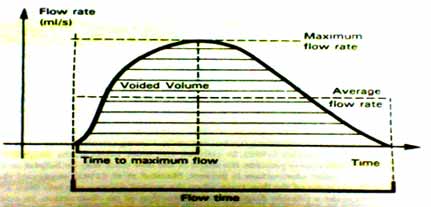
- Flow rate volume of urine through urethra per unit time, expressed in ml/sec.
- Peak flow rate (Q Max) maximum measured flow rate.
- Voided volume total volume expelled through urethra.
- Flow time Total time over which measurable flow occurs.
- Average flow rate voided volume / flow time.
- Time to maximum flow elapsed time from onset of flow to maximum flow.
- Intermittent flow flow time should be measured carefully. The time intervals between the flow episodes are disregarded.
Indications
- Possible bladder outlet obstruction / symptoms of outlet obstruction.
- Women subjected to undergo surgery for stress incontinence.
- Elderly women to exclude residual urine, a cause of recurrent UTI.
- Pre-operative workup and post-operative follow up in case of urethral stricture, Benign Prostatic Hyperplasia (BPH) bladder neck obstruction.
Equipment
Most commercially available flow-meters have acceptable accuracy. Three types popular -
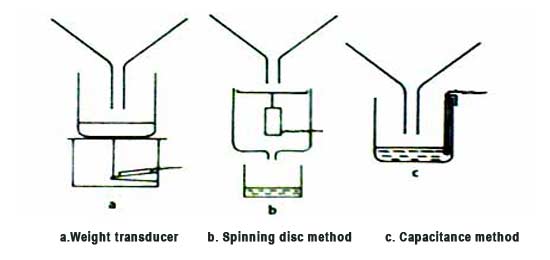
- Weight transducer flow meter Weighs the urine voided - measuring the volume of urine voided and hence the urine flow rate by differentiation with respect to time.
- Ordinary pressure transducer The hydrostatic pressure exerted by a column of urine also can be applied to measure the weight of the urine voided.
- Rotating disc flow meter Has a spinning disc on which urine falls.
The disc rotates at a same speed by a servomotor, in spite of changes in the urine flow rate.
The weight of urine tends to slow the disc speed.
The differing power needed to maintain disc rotation constant is proportion to the urine flow rate.
Urine flow clinics
- Uroflow studies should be performed in privacy when the patient has a normal desire to void and is relaxed.
- Patient is asked to drink 500 ml to 1 litre of fluid on arrival. They are asked to hold their urine until comfortably full - but not bursting to pass urine.
- Then patient is led into the flow room, having been made familiar about the equipment, the person is allowed to pass urine in privacy.
- Ideally 3 flows to be recorded on three occasions and each time after passing urine, their post-void residual urine recorded ultrasonographically.
Normal flow patterns
- A variety of normograms has been produced by various authorities, such as Von Garrelts (1958), Backman (1965), Gierup (1965), Siroky et al (1979), Kadow et al (1985) and Haylen (1990).
- The shape of the curve is unimodal i.e. monotonic increase, stable period, monotonic decrease.
- Bell shaped.
- Maximum flow is reached in first 30% of any trace and within 5 seconds (3-10 S) from the start of the flow.
- The flow rate may vary with amount of urine voided.
- The final phase of a normal flow trace shows a rapid fall from high flow, with a sharp cut off at the termination of the flow.
- The trace appearance may vary with paper speed. A paper speed of 25 cm/s is recommended.
- Urine flow rate is highly dependent on the volume voided.
- Flow rates are highest and more predictable with 200-400 ml urine volume.
- Detrusor muscle when stretched achieves an optimal performance, but when stretched further it becomes inefficient (> 400ml).
- Uroflow in an adult male is considered to be normal if it is bell shaped with a peak flow of 15 ml/sec or more on more than one occasion.
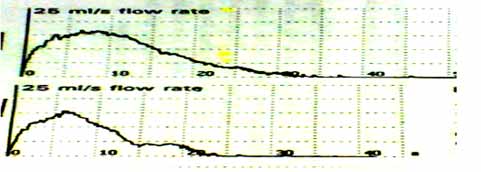
- Normally Uroflow in an adult female should be bell shaped with a peak flow rate of 25ml/sec
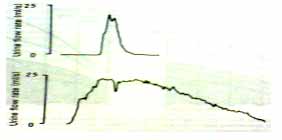
Similar peak flow rate or Q max but different flow curve shapes due to different voided volumes are shown below.
AHCPR Guidelines
- Flow rate measurements are inaccurate if the voided volume is less than 125 to 150 ml.
- Flow rate recording is the single best noninvasive urodynamic test to detect lower urinary tract obstruction. However there is no recommended "cut-off" value.
- The peak flow rate (PFR; Qmax) more specifically identifies patients with BPH than does the average flow rate (Qave).
- Although Qmax decreases with advancing age and decreasing voided volume, no age or volume correction is currently recommended for clinical practice.
- Patients with a Qmax > 15 ml/sec appear to have somewhat poorer treatment outcomes after prostatectomy than patients with a Qmax < 15 ml/sec.
- A Qmax of less than 15 ml/sec does not differentiate between obstruction and bladder decompensation.
- Age: 4 to 7
- The average flow rate for both males and females is 10 mL/sec.
- Age: 8 to 13
- The average flow rate for males is 12 mL/sec.
- The average flow rate for females is 15 mL/sec.
- Age: 14 to 45
- The average flow rate for males is 21 mL/sec.
- The average flow rate for females is 18 mL/sec.
- Age: 46 to 65
- The average flow rate for males is 12 mL/sec.
- The average flow rate for females is 15 mL/sec.
- Age: 66 to 80
- The average flow rate for males is 9 mL/sec.
- The average flow rate for females is 10 mL/sec.
- Artifacts can occur from abdominal straining or "waggling" of the stream.
Detrusor over activity
- Supra-normal pattern. Very high maximum flow rate may be achieved with an abnormally short time of 1-3 secs.
- The detrusor contraction may have already opened the bladder neck widely thus reducing the urethral resistance. Hence he/she is required only to relax the distal sphincter.
Bladder Outflow Obstruction (BOO)
- The flow curve has low maximum flow and also reduced average flow rates, with the Qave being more than half the Qmax.
- Maximum flow may be obtained quickly (3-10S) but the final phase decreases slowly.
- The obstruction may be compressive (BPH) or constrictive (urethral stricture).
BPH
- Shows a compressive pattern, the first third of the curve may appear normal, Qmax may be reduced.
- The final phase is elongated into a pronounced tail of reducing flow rate.
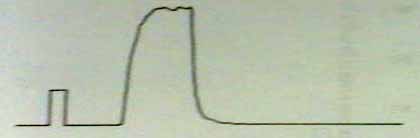
Stricture
- The later produces a plateau - shaped curve, with very meagre difference between Qmax and Qave.
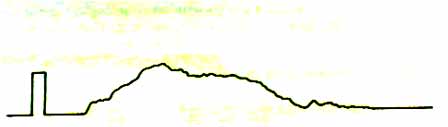
Detrusor under-activity
- Produces low maximum flow rate.
- The time to reach the maximum flow is variable and usually occurs in the second half of the curve.
- The traces of both obstruction and detrusor under-activity may look similar, making it difficult to distinguish between the conditions.
- Requires urodynamic pressure flow study.
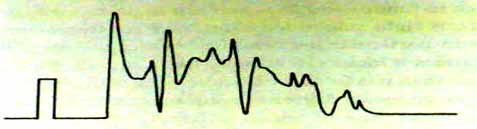
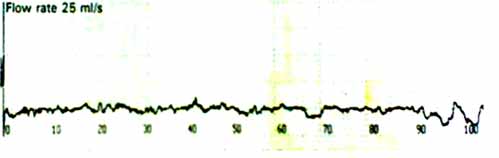
 Irregular interrupted flow patterns
Irregular interrupted flow patterns - May occur secondary to straining in cases of obstruction or detrusor hypocontractility.